Avoiding Injury: Prehab for Shoulders and Lower Back
Bulletproof Your Joints: Shoulder & Lower Back Prehab
Push/Pull Ratio Assessor
Enter your strict 5–8 rep working weights to detect hidden muscular imbalances and immediately assess your acute risk of shoulder impingement.
The pursuit of peak hypertrophy and maximal strength in natural bodybuilding is a multi-decade endeavour that demands more than just intensity in the weight room and precision in the kitchen. For the drug-free athlete, the physiological ceiling is governed by endogenous hormonal recovery and, more critically, the structural integrity of the connective tissues. Bodybuilding injury prevention is not merely a defensive strategy; it is the absolute prerequisite for long-term progression and sustained tissue overload. Unlike the musculature, which possesses high vascularity and a robust capacity for rapid remodeling, the joints—specifically the complex architectures of the shoulder and the lumbar spine—are subjected to cumulative mechanical stress that often outpaces their biological repair rates. Nearly every serious resistance trainee will encounter rotator cuff impingement or lumbar discogenic pain at some stage of their career if they push the boundary of strength. This report provides an exhaustive, expert-level analysis of the biomechanical mechanisms underlying these prevalent injuries and offers a comprehensive prehabilitation (prehab) framework designed to optimize joint resilience, structural density, and ensure absolute athletic longevity.
Biomechanical Pathophysiology of the Shoulder Complex
The human shoulder is an evolutionary masterpiece of mobility, yet its vast range of motion is achieved at the direct expense of intrinsic stability. The glenohumeral joint is frequently described as a “ball-and-socket” joint, though biomechanically, it more closely resembles a golf ball sitting on a tee, where the humeral head is significantly larger than the glenoid fossa of the scapula. This anatomical vulnerability places an immense burden on the rotator cuff muscles—the supraspinatus, infraspinatus, subscapularis, and teres minor—to maintain dynamic stability through a mechanism known as concavity compression.
Mechanisms of Subacromial and Internal Impingement
Shoulder impingement syndrome is not a singular diagnosis but a spectrum of pathologies characterised by the compression of soft tissues within the shoulder’s restricted corridors. Research indicates that shoulder impingement constitutes approximately 74% of all clinical shoulder pain cases in strength athletes. In the context of heavy resistance training, this impingement is typically categorised into external and internal types, each with distinct mechanical triggers.
External impingement, or subacromial impingement, occurs when the bursal side of the rotator cuff tendons (most commonly the supraspinatus) is compressed against the coracoacromial arch. This space is naturally narrow, spanning only 1.0 to 1.5 cm. Any reduction in its height—whether through inflammation, bony abnormalities (acromial spurs), or poor lifting mechanics—leads to the mechanical abrasion of the tendon. For natural bodybuilders, this often manifests during exercises involving internal rotation under load, such as the upright row or improperly executed lateral raises. In these movements, the greater tuberosity of the humerus migrates superiorly and pinches the subacromial tissues.
Internal impingement describes the entrapment of the articular side of the supra- or infraspinatus tendons between the humeral head and the glenoid rim. This phenomenon is particularly prevalent in the “late cocking” or “catch” positions of explosive lifts, or during the deep eccentric portion of a heavy bench press, where the shoulder is in a state of maximal abduction and external rotation. The repetitive entrapment of these tissues leads to fraying, tendinopathy, and eventual labral tears.
| Impingement Category | Primary Tissue Affected | Mechanical Context | Typical Training Trigger |
|---|---|---|---|
| Subacromial (External) | Bursal side of Supraspinatus | Compression under acromion | Upright rows, internal rotation |
| Internal (Posterior) | Articular side of Infra/Supraspinatus | Entrapment against glenoid rim | Deep bench press, snatch catch |
| Coracoid Impingement | Subscapularis tendon | Compression against coracoid process | Forced horizontal adduction |
Case Study: The “Bencher’s Shoulder” Phenomenon
Consider a granular case study of a competitive natural bodybuilder executing a 140kg bench press peaking cycle without integrated shoulder prehab. After week four, chronic anterior deltoid pain presented during the initial descent of the bar. Clinical assessment revealed a combination of type II dyskinesis (prominent medial scapular border) and subacromial impingement.
The physiological analysis was simple yet devastating: a hyper-dominant pectoralis major and latissimus dorsi pulled the humeral head anteriorly and internally. Concurrently, an underactive lower trapezius and serratus anterior failed to posteriorly tilt the scapula during the lift. The result? A 3mm reduction in the subacromial space. Over hundreds of repetitions, this caused chronic supraspinatus micro-tearing. Incorporating daily face pulls and banded “Y” raises resolved the impingement entirely within eight weeks by physically altering the resting posture of the scapula.
The Scapulohumeral Rhythm and Dyskinesis
Optimal shoulder function is predicated on the “scapulohumeral rhythm,” a coordinated 2:1 ratio of movement between the humerus and the scapula. For every 2 degrees of humeral elevation (abduction or flexion), the scapula must upwardly rotate by 1 degree to maintain the subacromial space. In many lifters, this rhythm is disrupted by “scapular dyskinesis”—an alteration in the normal position or motion of the scapula during humeral movement.
Dyskinesis is frequently driven by muscular imbalances common in bodybuilding: hyper-dominant internal rotators coupled with inhibited or weak scapular stabilisers. When the scapula fails to upwardly rotate and posteriorly tilt during an overhead press or bench press, the acromion remains “in the way,” causing the humerus to strike the subacromial structures prematurely. Research suggests that even small deviations in scapular kinematics can lead to increased humeral head anterior and inferior translation, further destabilising the joint.
Lumbar Spine Biomechanics and Force Distribution in Heavy Lifting
The lumbar spine is the foundational pillar of the human frame, tasked with transferring massive forces between the lower and upper body during the “Big Three” lifts (squat, bench press, deadlift). In powerlifting and bodybuilding, the lumbar region (L1–L5) is the most frequently injured area, representing 28–59% of all reported spinal injuries.
Compressive and Shear Loading in the Deadlift
Heavy compound pulling, specifically the deadlift, exposes the lumbar vertebrae to extreme mechanical loads. Studies utilising motion capture and force plate data have quantified these loads, revealing that 1RM efforts can produce compressive forces ranging from 5,000 to 18,000 Newtons (kN) and shear forces between 1.3 and 3.2 kN. To contextualise these figures, 18 kN is roughly equivalent to the weight of a small car being supported by the five lumbar vertebrae.
The distribution of these forces is not uniform. The L4/L5 and L5/S1 segments bear the brunt of the load. During the initial “break” of a deadlift from the floor, the net moment at the L4/L5 joint can range from 445 Nm to 1,071 Nm in experienced male lifters. This moment must be countered by the spinal erectors and the intra-abdominal pressure (IAP) generated through a proper “brace” or “valsalva maneuver.”
Advanced Granular Load Analysis: Minute-by-Minute Deadlift Torque
During a heavy conventional deadlift, the torque applied to the lower back follows a steep gradient.
- 0.0 - 0.5s (The Setup): The lifter takes slack out of the bar. Spinal erectors fire at 30-40% maximal voluntary isometric contraction (MVIC). Compressive forces sit around 2,000 N. Intra-abdominal pressure hits 100 mmHg.
- 0.5 - 1.2s (The Break): The load breaks the floor. The moment arm at L5/S1 reaches its absolute peak. Erector spinae output spikes to 100% MVIC. Compressive forces exceed 12,000 N depending on absolute load. Shear forces, if the spine mildly flexes, spike to an alarming 2.5 kN.
- 1.2 - 2.5s (The Lockout): As the hips extend, the moment arm shortens. Compressive force is high, but the dangerous anterior shear force plummets as the torso angle becomes vertical. Gluteal output overrides erector demand.
When the lifter performs a straight-leg deadlift (or Romanian deadlift), the torque curve changes drastically. The hips remain high, extending the moment arm significantly during the transition phase.
| Metric | Traditional Deadlift | Hexagonal Bar Deadlift | Straight-Leg Deadlift |
|---|---|---|---|
| Lumbar Flexion Angle | 58° | 55° | 90° |
| Peak Lumbar Torque | 749 N·m | 640 N·m | 893 N·m |
| L5 Vertebral Stress | ~750 MPa | ~600 MPa | 997 MPa |
| Trabecular Bone Stress | ~2.5 MPa | ~2.1 MPa | 3.3 MPa |
The data indicates that the straight-leg deadlift pushes the L5 vertebral body to a peak stress of 997 MPa, which is dangerously close to the acute damage threshold of 1,000 MPa. Furthermore, the trabecular bone stress in this movement (3.3 MPa) exceeds the fatigue failure threshold of 3.0 MPa, suggesting that high-volume, straight-leg pulling is a primary driver of stress fractures (spondylolysis) in the lumbar region.
Specific Bone-Density Adaptation Formulas for Natural vs. Enhanced Populations
One of the most misunderstood aspects of bodybuilding injury prevention is the disparity in bone remodeling between natural and enhanced lifters. Cortical and trabecular bone density increases according to Wolff’s Law, which states that bone adapts to the mechanical loading placed upon it. The mathematical remodeling rate ($R$) is largely dictated by mechanical strain ($\epsilon$) and the hormonal environment ($H$).
For a natural lifter, the osteogenic adaptation formula roughly follows: $R = (\epsilon imes f) imes H_{nat}$ Where $f$ is the frequency of loading, and $H_{nat}$ is the physiological baseline of free testosterone and IGF-1. Natural bone remodeling is an incredibly slow process. If a natural bodybuilder increases deadlift volume by 40% in a month, the musculature may adapt, but the bone matrix incurs a net loss in mineral density (a negative modeling phase) before it super-compensates months later.
Conversely, for an enhanced lifter utilising exogenous androgens (such as Nandrolone or robust doses of exogenous Testosterone), $H_{enh}$ creates an artificially hyper-accelerated remodeling window. Enhanced athletes synthesise collagen and deposit calcium at a severely accelerated rate, masking the symptoms of mechanical overload right up until catastrophic failure occurs. The natural lifter cannot risk this; their loading parameters must respect the biological timeline of human osteoblasts and osteoclasts, which operate strictly on a three-to-four month physiological cycle.
Discogenic Pain vs. Herniation
Lumbar discogenic pain, which accounts for nearly 40% of low back issues in strength athletes, is distinct from a traditional disc herniation. It involves the mechanical or chemical irritation of the nerves within the fibrous outer ring (annulus fibrosus) of the disc without necessarily involving a protrusion of the gel-like center (nucleus pulposus).
This pain is typically exacerbated by sustained flexion (rounding the back) under load. When the spine flexes, the vertebrae squeeze the front of the disc, pushing the nucleus pulposus backward against the sensitised nerves of the annulus. If the core musculature fails to maintain “stiffness,” the gel overcomes the strength of the fibrous tissue, leading to a “disc sprain” or chemical inflammation.
The Science of Prehabilitation: Neuromuscular Foundations
Prehabilitation is a proactive, evidence-based strategy designed to increase an athlete’s “functional reserve”—the gap between their current physical capacity and the demands of their sport. For the natural bodybuilder, prehab is not an “optional” addition but a necessary countermeasure to the wear-and-tear of high-intensity training.
Neuromuscular Adaptation Timelines
A critical finding in prehabilitation research is that meaningful changes in joint stability and injury risk reduction require a minimum of 12 weeks of consistent intervention. This timeline is necessary for both neurological adaptation (improving motor unit recruitment and co-contraction) and structural remodeling (increasing the cross-sectional area and stiffness of tendons and ligaments).
Systematic reviews encompassing over 5,000 athletes have demonstrated that structured prehab programs can significantly reduce the incidence of acute injuries, such as muscle strains and ligament tears, and diminish the severity of chronic overuse conditions. The efficacy of these programs is rooted in three primary mechanisms:
- Proprioceptive Enhancement: Improving the brain’s awareness of joint position to prevent “micro-movements” that lead to impingement or nerve irritation.
- Muscle Balance Restoration: Targeting “inhibited” muscles like the lower trapezius or multifidus to take the strain off the joints.
- Joint Stabilisation: Training the surrounding musculature to act as a “dynamic sleeve,” compressing the joint and maintaining optimal alignment under load.
Advanced Shoulder Prehabilitation Protocols
To “bulletproof” the shoulder, the natural bodybuilder must address the primary deficits found in most lifters: poor thoracic mobility, weak external rotators, and inhibited scapular retractors.
The Face Pull: Mechanics and Variations
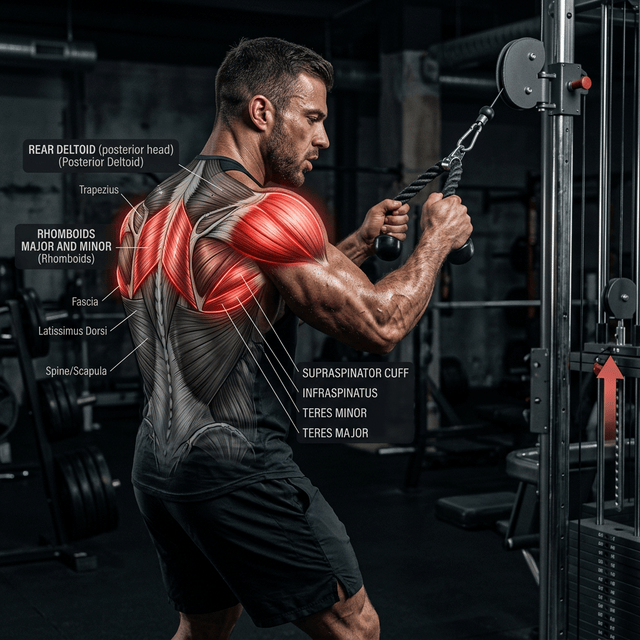
The face pull is widely regarded by sports scientists as the most effective “all-in-one” shoulder prehab exercise. It addresses the systematic imbalances caused by excessive horizontal pressing (bench press) by strengthening the rear deltoids, rhomboids, middle trapezius, and the external rotators (infraspinatus and teres minor).
The face pulls benefits extend far beyond aesthetics. The intent of the face pull is to force external rotation while simultaneously retracting the scapulae, offsetting the kyphotic posture built from heavy pressing. Research indicates that different anchor heights yield specific benefits:
- High-to-Low Face Pull: Anchoring the cable above head height increases the demand on the lower trapezius and scapular depressors, helping to “pull the shoulders down” away from the ears.
- Parallel (Eye-Level) Face Pull: Emphasises the rear deltoids and horizontal abduction, providing the purest force vector for scapular retraction.
- Low-to-High (Chest-Level) Face Pull: Focuses heavily on the infraspinatus and teres minor, maximising the external rotation component.
For optimal results, face pulls should be performed 2–3 times per week for 3–4 sets of 12–15 repetitions. The focus must remain on “pulling the rope apart” and holding the terminal contraction for 1–2 seconds to build postural endurance.
Minute-by-Minute Protocols for the 12-Week Prehab Cycle
Integrating a rotator cuff warm up and lumbar support system cannot be done haphazardly. The elite execution follows a strict 12-week undulating progression matrix designed to shift from neurological priming to structural endurance.
Weeks 1-4: Proprioceptive and Iso-Metric Integration
- Minute 0:00 - 2:00: The McGill Curl-Up. 5 reps of 10-second high-tension isometric holds per side.
- Minute 2:00 - 4:00: The Side Plank. 4 reps of 10-second maximum tension holds per side, aggressively contracting glutes.
- Minute 4:00 - 6:00: The Bird Dog. 5 reps per side, 10-second extreme tension holds, pressing the heel out to activate the gluteus medius.
- Minute 6:00 - 8:00: Thoracic Foam Roller Extensions. T6-T8 region opening.
- Minute 8:00 - 10:00: High-to-Low Cable Face Pulls. 2 sets of 15 reps, 2-second isometric squeeze at maximal external rotation.
Weeks 5-8: Kinetic Linking and Eccentric Control
- Shift from pure isometrics to slow-eccentric movements. Face pulls are now performed with a 4-second eccentric (negative) phase to force tendon thickening.
- Incorporate decompression exercises like dead-hangs from a pull-up bar for 60 seconds post-workout to rehydrate the intervertebral discs and decompress the glenohumeral joint capsule.
Weeks 9-12: Dynamic Load Preparedness
- The core braces (McGill Big Three) are executed immediately before heavy working sets at a 3-rep, 10-second hold paradigm.
- Face pulls transition to parallel height at a heavier load, 3 sets of 10 reps, solidifying strength in extreme ranges of posterior chain motion.
Thoracic Spine Mobility: The Missing Link
A rigid thoracic spine (T1–T12) is often the root cause of shoulder impingement. To elevate the arms overhead without compensation, the human body requires approximately 10° of thoracic extension and 50–55° of thoracic rotation. When the thoracic spine is “locked” into a kyphotic (hunched) position—common in modern sedentary lifestyles—the scapula cannot posteriorly tilt or upwardly rotate, leading to immediate subacromial impingement during pressing.
Lifters can utilise the “Thoracic Extension Test” to identify limitations: sitting with the back flat against a wall and attempting to raise the arms overhead without the lower back arching or the head moving forward. If the hands cannot touch the wall, a thoracic mobility protocol is mandatory.
Lumbar Resilience and the “Stiffness” Paradigm
In the realm of lumbar prehabilitation, the goal is not to increase flexibility but to cultivate “stiffness.” Dr. Stuart McGill, a world-renowned spinal biomechanist, defines stiffness as the co-contraction of the musculature to arrest painful vertebral micro-movements. This stiffness transforms the torso into a rigid, load-bearing cylinder, protecting the sensitive discs and nerves of the lumbar spine and preventing lower back pain deadlift scenarios.
The McGill Big Three: Neurological Priming
The “McGill Big Three” is a triad of exercises specifically designed to build core stability and endurance without placing the spine under heavy compressive loads. These are not “ab exercises” in the aesthetic sense; they are neurological drills intended to “prime” the nervous system to maintain a neutral spine under load.
1. The Modified Curl-Up The intent of the McGill Curl-Up is to stiffen the anterior core without bending the lumbar spine.
- Execution: Lie on the floor with one leg straight and the other bent. Place hands under the small of the back to maintain a neutral curve. Lift the elbows off the floor. Instead of “crunching” forward, imagine the head is on a scale and you want the scale to read “zero.” Lift the head and shoulders just 1–2 inches off the floor and hold for 10 seconds.
- Key Insight: This teaches the rectus abdominis and obliques to fire in a way that locks the ribcage to the pelvis.
2. The Side Plank The side plank targets the quadratus lumborum and obliques, which are the primary lateral stabilisers of the spine.
- Execution: Bridge from either the knees or the feet, maintaining a perfectly straight line from head to heel. The intent is to teach the “hip hinge” in a stable position and fire the glutes and core together as a unified system.
- Key Insight: This exercise “breaks the mental cycle of fearing forward bending” by providing a safe context for core engagement.
3. The Bird Dog The bird dog is a full-body stability movement that challenges the lifter’s ability to prevent spinal rotation.
- Execution: From a quadruped (tabletop) position, extend the opposite arm and leg. The goal is to keep the spine and hips perfectly level. Cues like “punching a hole in the wall” with the fist and “kicking the wall” with the heel maximise tension.
- Key Insight: This drill works the posterior chain (multifidus, erector spinae, glutes) while training the limbs to move independently of the spine.
Programming Core Stiffness
Research indicates that long-term isometric training (like the Big Three) is superior to dynamic core training (like crunches) for enhancing active core stiffness. To maximise neurological priming without exhausting the muscles, these should be programmed in a “reverse pyramid” fashion (e.g., 5 reps, then 3, then 1), with each rep being a 10-second high-intensity hold.
Nutritional Biochemistry for Joint and Tendon Integrity
For the natural bodybuilder, nutrition is the only variable that can accelerate the traditionally slow recovery of connective tissues. Connective tissues—tendons, ligaments, and cartilage—possess significantly lower metabolic rates and blood flow than muscle tissue, often requiring specific nutrient “loading” to facilitate repair.
Detailed Chemical Pathways of Amino Acid Hydroxylation
Collagen is the most abundant structural protein in the human body, comprising 65–80% of the dry weight of tendons. It is characterised by phenomenally high concentrations of the amino acids glycine, proline, and hydroxyproline. The sheer tensile strength of tendons relies directly on the chemical cross-linking of these amino acid chains into a robust triple-helix structure.
This is where the biochemistry becomes critical for natural athletes. To form this structure, the body must convert standard proline and lysine into hydroxyproline and hydroxylysine. This conversion is driven by the enzymes prolyl hydroxylase and lysyl hydroxylase.
Here is the exact biochemical cascade:
- The athlete consumes 15g of hydrolysed collagen peptides 60 minutes prior to training.
- The peptides are broken down to high levels of systemic glycine and proline.
- The athlete pairs this ingestion with 50-500mg of Vitamin C (Ascorbic Acid).
- Ascorbic acid acts as a mandatory electron donor in the active site of prolyl hydroxylase. It reduces the iron center in the enzyme from its inactive ferric state (Fe3+) back into its active ferrous state (Fe2+).
- Only then can the enzyme attach a hydroxyl group (-OH) to the proline ring.
- The resulting hydroxyproline tightly winds the protein chains, dramatically enhancing the thermal stability and tensile force resistance of the rotator cuff and spinal erector tendons.
Attempting to repair micro-tears in connective tissue without adequate ascorbic acid to facilitate this pathway fundamentally halts the structural healing process and leads to weak, haphazard scar tissue formation.
Practical Collagen Supplementation for Natural Athletes
While collagen is effective for joint health, it is a “poor” protein source for muscle growth because it lacks the essential amino acid tryptophan and is low in leucine. Therefore, it should be treated as a “joint supplement” rather than a primary protein source.
| Supplement Type | Dose | Goal | Timing |
|---|---|---|---|
| Hydrolysed Collagen | 5–15 g | Joint function/pain reduction | 60 min pre-workout |
| Vitamin C | 50–500 mg | Facilitate collagen cross-linking | Co-ingested with collagen |
| Whey Protein | 25–40 g | Muscle protein synthesis | Post-workout |
For natural athletes, maintaining a total daily protein intake of 1.6–2.2g per kilogram of body weight is the baseline for both muscle and joint health. However, those prone to injury or on plant-based diets may need to prioritise glycine-rich foods or specific collagen supplementation to offset the higher “collagen breakdown” caused by heavy mechanical tension.
Debunking Prevalent Bodybuilding Myths
Longevity in the gym is often hindered by “bro-science” and outdated instructional paradigms. Scientific inquiry has recently debunked several myths that contribute to injury or unnecessary movement restrictions.
Myth 1: “Never Let Your Knees Go Past Your Toes”
This myth originated from a 1978 study which found that restricting forward knee movement reduced knee stress. However, modern research demonstrates that by restricting the knees, the lifter is forced to lean further forward, which increases hip and lumbar stress by nearly 1,000%. Allowing the knees to travel beyond the toes is a normal anatomical function seen in children and elite athletes; it is essential for a deep, balanced squat and for distributing load evenly across the kinetic chain without overloading the lower back.
Myth 2: “Rounding Your Back is a Guaranteed Disc Herniation”
While uncontrolled flexion under maximal load is risky, the human spine is designed to flex. In fact, the average person flexes their spine up to 2,000 times a day. Research on elite rowers shows they load their spines in a flexed position without an epidemic of injury because their tissues have undergone “graded exposure” and adaptation. For bodybuilders, the goal is to maintain a “neutral” spine for maximal attempts, but training the spine to handle light flexion increases resilience against sudden, unexpected movements.
Myth 3: “Stretching the Lower Back Relieves Tightness”
Many lifters experience a “tight” lower back and respond by performing toe-touches or “knee-to-chest” stretches. However, if the tightness is caused by a discogenic issue or core instability, stretching the lumbar spine can actually increase nerve irritation and disc pressure. In most cases, the lower back is tight because it is trying to provide stability that is lacking elsewhere. The solution is not to stretch the back, but to mobilise the hips and thoracic spine while stabilising the lumbar.
Myth 4: “Steroid Users and Naturals Can Train the Same Way”
Natural bodybuilders rely entirely on “mechanical tension” and “progressive overload” to drive hypertrophy. Enhanced athletes, aided by artificially high protein synthesis and recovery, can utilise extreme volumes and shorter rest periods. For the natural lifter, attempting “enhanced” volumes often leads to systemic overtraining and connective tissue failure, as the joints cannot recover at the same rate as chemically-assisted muscles.
Practical Integration: The Bulletproof Training Week
To transition from theory to practice, the prehab protocols must be woven into the lifter’s existing routine. The following “Natural Athlete’s Joint Longevity Program” provides a blueprint for daily and weekly integration.
The 10-Minute Daily “Spinal Hygiene” Routine
This should be performed every morning or prior to every workout to “stiffen” the core and mobilise the upper back.
- Cat-Camel (8–10 reps): Gentle, unweighted spinal flexion and extension to “floss” the nerves and hydrate the discs.
- McGill Big Three (1–2 sets): 10-second holds in a reverse pyramid (5-3-1) to prime the neurological “brace”.
- Thoracic Foam Rolling (2 minutes): Focused extension over the roller to unlock the upper back.
The Pre-Workout Shoulder “Primer”
Performed specifically before any “Push” or “Upper Body” session.
- Face Pulls (2 sets of 15): Light weight, focusing on external rotation and scapular retraction.
- Banded Wall Slides (10 reps): Pressing the forearms into the wall to activate the serratus anterior and lower trapezius.
- Doorway Chest Stretch (30 seconds): Reducing tension in the pectoralis minor to allow for better scapular tilting.
Managing Volume and Intensity for Longevity
Natural athletes must manage “Total Joint Load.” Research on powerlifting injuries indicates that while the absolute 1RM is stressful, it is the “repetitive heavy loading” (80%+ 1RM) that often leads to fatigue failure in spinal and shoulder tissues.
- Autoregulation: Using RPE (Rate of Perceived Exertion) or RIR (Repetitions in Reserve) to avoid training to total failure on every set. This minimises “technique breakdown,” which is when the majority of acute disc and labral injuries occur.
- De-load Weeks: Every 4–6 weeks, reducing training volume by 50% allows the slow-recovering connective tissues to “catch up” to the faster-recovering muscles.
Conclusions and Future Outlook
The “bulletproof” joint is not an anatomical accident but a product of deliberate, science-backed engineering. For the natural bodybuilder, injury prevention is synonymous with progress. By understanding the biomechanical stress thresholds—such as the 1,000 MPa limit of the L5 vertebra or the 2:1 scapulohumeral rhythm—the athlete can make informed decisions about exercise selection and execution.
The synthesis of current research emphasises that joint longevity is built on three pillars:
- Neuromuscular Integrity: Using drills like the McGill Big Three and face pulls to ensure the joints are supported by active muscular “stiffness”.
- Biomechanical Awareness: Avoiding high-risk positions like straight-leg deadlifts under maximal load and maintaining thoracic mobility to protect the shoulders.
- Nutritional Support: Leveraging the synergistic effects of collagen, Vitamin C, and mechanotransduction to promote the structural remodeling of tendons and ligaments.
As natural bodybuilding continues to grow, the integration of these “prehab” protocols will separate the elite, long-term athletes from those whose careers are cut short by preventable joint failure. The data is clear: 12 weeks of dedicated prehabilitation can transform a vulnerable joint into a resilient structure capable of withstanding the inevitable wear-and-tear of heavy lifting, keeping the athlete “under the bar” for decades to come.
Frequently Asked Questions
1. Is subacromial impingement permanent? No. Subacromial space reduction is typically a mechanical issue driven by muscular imbalance (tight internal rotators, weak lower trapezius) or poor posture. By executing a strict 12-week prehab protocol combining face pulls and thoracic mobility work, natural bodybuilders can successfully recenter the humeral head and eliminate the friction causing the pain.
2. Why do straight-leg deadlifts cause more lower back pain than conventional deadlifts for some lifters? Biomechanically, the moment arm connecting the load to the lumbar spine is severely extended when the hips remain exceptionally high. This forces peak L5 vertebral stress to roughly 997 MPa, dramatically increasing trabecular bone fatigue. Natural athletes must autoregulate the volume of heavily loaded hinging movements or they risk stress fractures.
3. Does supplementing with Vitamin C and collagen directly repair tendons? Systemic evidence indicates that consuming 15g of hydrolysed collagen paired with 50mg of Vitamin C precisely 60 minutes before training significantly amplifies the blood markers of collagen synthesis. The Vitamin C drives the enzymatic hydroxylation of proline, physically strengthening the cross-link integrity within the connective tissue matrix.